Mixed Race Infants are Unhealthy Because of Complex Gene-Environment Interaction
The goal of abolishing the White race is on its face so desirable that some may find it hard to believe that it could incur any opposition other than from committed White supremacists. — Noel Ignatiev
1. Introduction
HEALTH DISPARITIES exist for infants in the United States, and this pattern can be recognized via racial/ethnic classification. This trend has been noticed in metropolitan areas like New York City. Borrell et al conducted a massive review via official health records for infants born in that area (Parental Race/Ethnicity and Adverse Birth Outcomes in New York City: 2000–2010). (4) Upon investigation, the researchers found minorities did have lower healthcare outcomes. Additionally, mixed infants are, in fact, unhealthier than White-monoracial children. I will be analyzing the data sets that they compiled because it was chiefly based on otherwise neutral sources. Because of how universally unhealthy mixed-race infants are, there must be genetic factors at play here. This article does not review the various cognitive problems that mixed children would suffer from via low birth-weight and preterm; that would require it’s own essay.(27) I must apologize ahead of time for the cut images; I was forced to separate the complete graphs in rows. This was because the data sets were too large. Additionally, I will address arguments that could be used against my thesis.
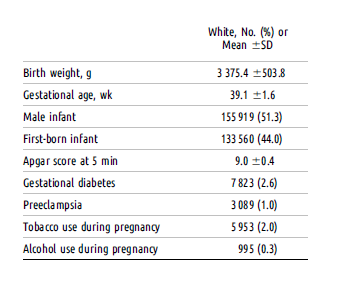
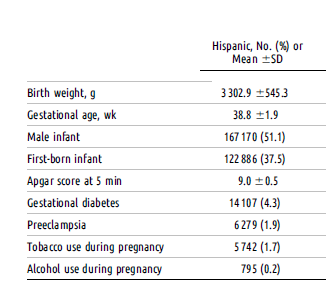
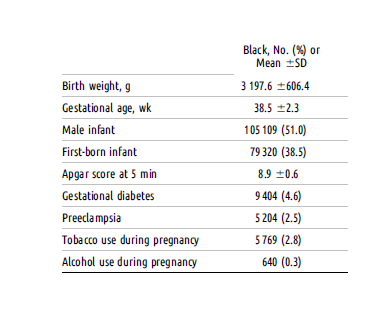
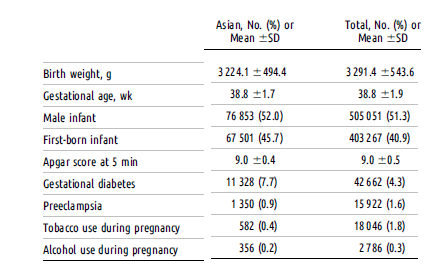
2. Relevant Datasets
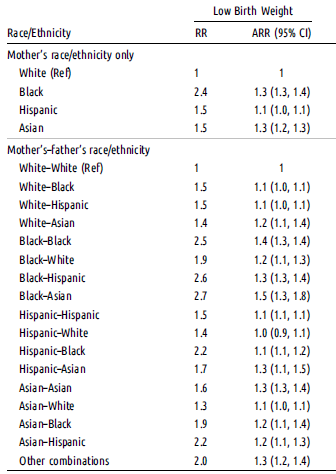
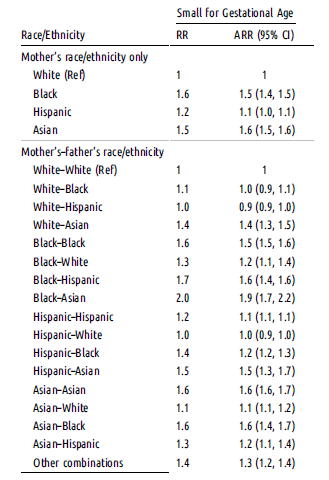
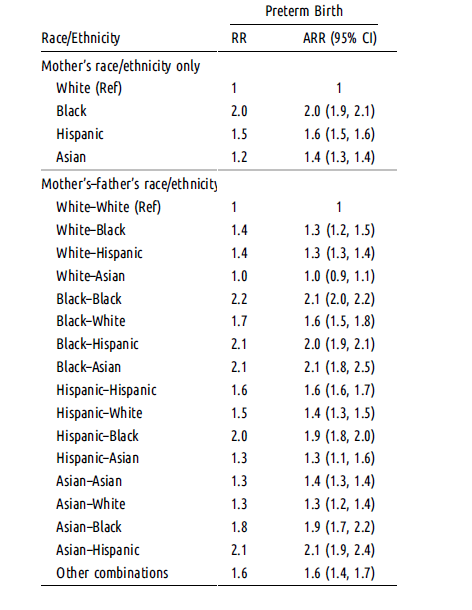
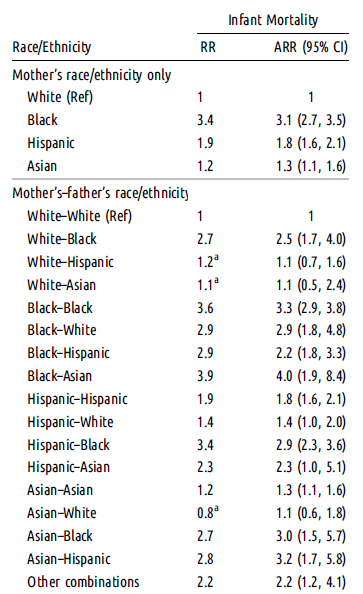
ARR = adjusted relative risk; CI = confidence interval; RR = relative risk;
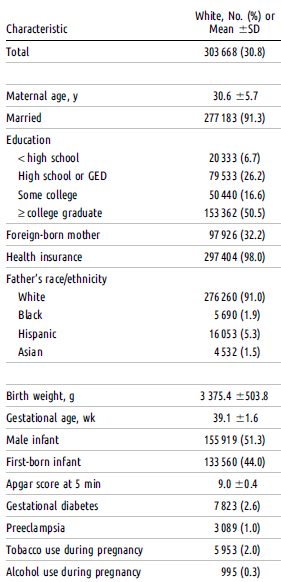
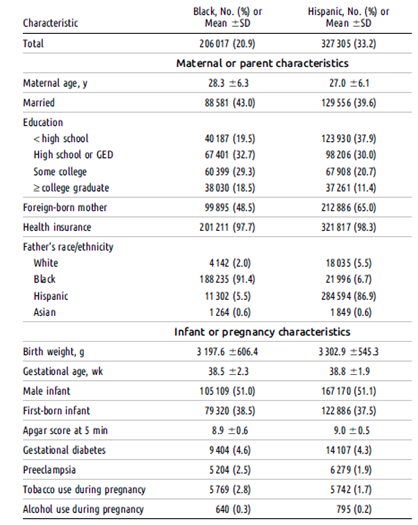
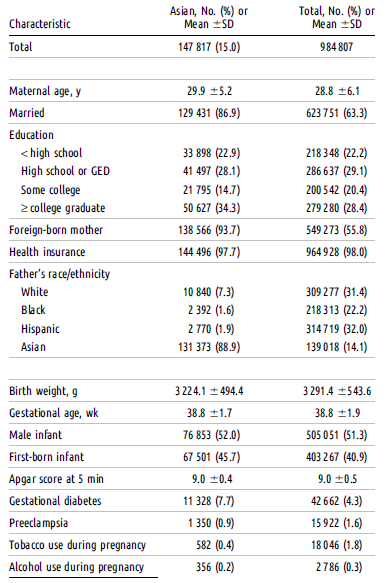
Relevant Socioeconomic Data For All Parents
3. Discourse/Explanation
The infant records were found via the Bureau of Vital Statistics of the NYC Department of Health and Mental Hygiene (DOHMH). These health records were matched with extreme accuracy. The researchers estimated that these records were 99% correct. Overall, 1,377,404 records were consulted. For the negative health ailments, the following standards were applied:
- Low-birth weight was considered under 2,500 grams (4)
- Gestational age was termed as “below the 10th percentile” (4)
- Preterm infants were born before 37 weeks (4)
- Infant mortality was defined as death in the first year (4)
The birth certificates described the race of each child. The researchers actually define interracial relationships as ethnic discordance, and I fully uphold this terminology. Any White person who is marrying outside of their group is technically committing an act discordance against their community; we need as many White people having healthy offspring (for reasons beyond the scope of this article).
The researchers themselves admit that White infants are considered the healthiest overall, “To account for concordance (parents of same race/ethnicity) and discordance (parents of different race/ethnicity), we created a variable combining mother’s and father’s race/ethnicity. We used Whites as the reference, as they have the lowest incidence for the study.”(4) Indeed, the researchers conclude that interracial relationships almost always produce unhealthier children regardless of the ailment, “We found that…there was increased risk of having an adverse birth outcome associated with having parents of different or discordant race/ethnicity, this increase was not consistent across outcomes and women’s race/ethnicity.”(4) This sentiment is reiterated at another time, “Moreover, compared with White couples, parental racial/ethnic discordance was associated with an increased risk of adverse birth outcomes for all racial/ethnic groups.”(4)
The only exception that can be found are White/Asian infants; they have the lowest rate of infant mortality (specifically at a rate of 0.8). However, these half-Asian infants suffer from preterm birth rates at a higher rate than monoracial, White infants (specifically at a rate of 1.3). This occurs when the father is White and the mother is Asian. Half-Asian infants are also more likely to suffer from low gestational weight (1.1) and low birth weight (1.1). Again, those ailments affect infants born to Asian mothers and White fathers. White men/Black females had high rates of low birth weight in their offspring (1.9). Hispanic females/White males produced a rate of 1.4 for low birth weight descendants.
What about other pairs? Infants born to Hispanic fathers and White mothers have a 1.5 higher risk of being born with a low birth weight. The exact same percentage was reported for infants descended from Black fathers and White mothers. Half-Asian infants that are descended from White mothers have a similar risk rate as well (1.4). Black females have terrible outcomes regardless of the partner. This is because of a whole host of factors which includes high drug abuse:”They are older, more likely to be black, and they have higher rates of illicit drug use, less education, and lower social status.”(13)
Asian males seem to have some of the worst outcomes for mixed infants, “For Black women, the risks of an adverse birth outcome were highest with an Asian partner.” This holds true for Hispanic women as well, “Hispanic women had greater risks of having a LBW or SGA baby with an Asian partner and higher risks of a preterm birth or IM with a Black partner.”(4) For White women and Asian males, their offspring were plagued with different health problems, “For example, we found that for White women, the risks of LBW and SGA were higher when they had an Asian partner…”(4) Asian women, who are known to marry outside their group at high levels in the United States, were demonstrated to have the worst outcomes for their offspring, “With the exception of no risk of IM when the father was White, Asian women’s risks were higher for all outcomes regardless of the father’s race/ethnicity, with the highest risks observed when the father was either Black or Hispanic.”(4)(30) Strong epigenetic evidence points to socioeconomic factors playing a role for gestational growth as well. King et al confirmed this in a comparison of infants from North Carolina.(15) So, there must be other epigenetic effects on infants in New York City that contribute to poor outcomes.
What about the rates of smoking and drinking among all ethnicities? It is apparent that, despite the fact that White infants are the healthiest overall, the rates of smoking and drinking are higher in White parents overall (the exception here would be Blacks).
Racial Smoking and Drinking Levels
How is it that minority infants are still unhealthy if their parents are smoking less than White parents? This is probably due to genetics and environment as well. A Dutch study compared the various rates of smoking among different ethnicities/races, “Since maternal smoking during pregnancy is quite equally distributed among the ethnic populations, it does not contribute much to the observed differences in birthweight.”(34) That study compared native Dutch people and immigrants.
Objection 1: How can you assume that the health problems associated with mixed race infants are partially genetic ? How do you know that stress and poverty aren’t the only/main culprits?
Borrel et al claim that a “weathering hypothesis” is the explanation for these poor outcomes.(4) However, the sources they cite were mainly deal with African American women only.(16)(17)(18) But that shall be addressed shortly. The poor health of interracial children was observed in early infant studies, “Group differences were more strongly related to the mother’s race than to the father’s, and the trends were related to the mother’s race. Because the father’s race was significant, genetic factors are probably of some importance.”(6) Later studies confirmed that genetic inheritance certainly played a significant role in a biracial infant’s health. But we need to look elsewhere: Gold et al found that significant health differences were found between White, biracial, and Black infants. The data came from California, and was based off health records from 1998-2002. The researchers found the following, “When all demographic, social, biological, genetic, congenital, and procedural risk factors except gestational age and birth weight were included, the odds ratios were all still significant. Black/black couples had the highest level of risk, followed by black mother/white father couples, and white mother/black father couples. Virtually all of the higher risk of fetal death was explainable by higher rates of low birth weight and prematurity.”(10) The compiled rates were as follows:
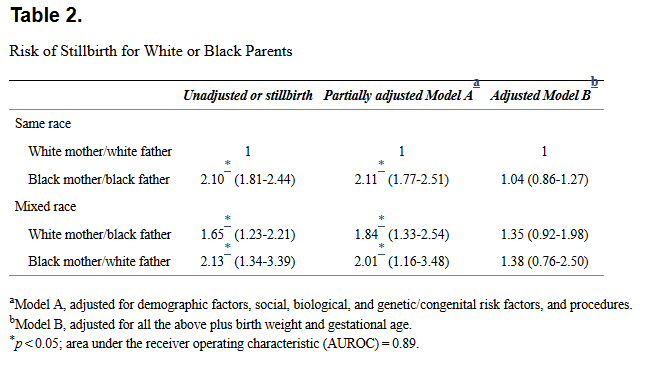
(Gold et al, 10)
As one can see, the amount of stillbirths was higher for the interracial couples. This was especially true of White father/Black mother relationships, but the White mother/Black father rates were still far worse than the rates of stillbirth for White couples. The outcomes for mulatto infants was at the detriment of the surveyed White population.(10)
What are the specifics to this horrible process? For this, we have to understand that having mixed genetic ancestry through mtDNA and yDNA perpetuates this happening. Let’s look at one of the best studies that has been published on this subject: “Divergent Patterns of Mitochondrial and Nuclear Ancestry Are Associated with the Risk for Preterm Birth.” This study investigated the unusually high rates of preterm birth among African Americans: “Haplogroup-defining polymorphisms are not merely markers of ancestry, and have consequences for mitochondrial function, including the regulation of mitochondrial gene expression.”(20)
Some might be surprised to know that many African Americans have large amounts of European ancestry. The European ancestry that African Americans have was distributed from White ,ales when slavery was still legal.(20) To put it another way, having ancestry from vastly different ancestors contributes to these genetic predispositions. It is necessary to demonstrate this with a principal component analysis. The turquoise dots below represent the African population. As one can see, the African American population is represented by a long cline between European American (CEU) and African (YRI) samples. (24)
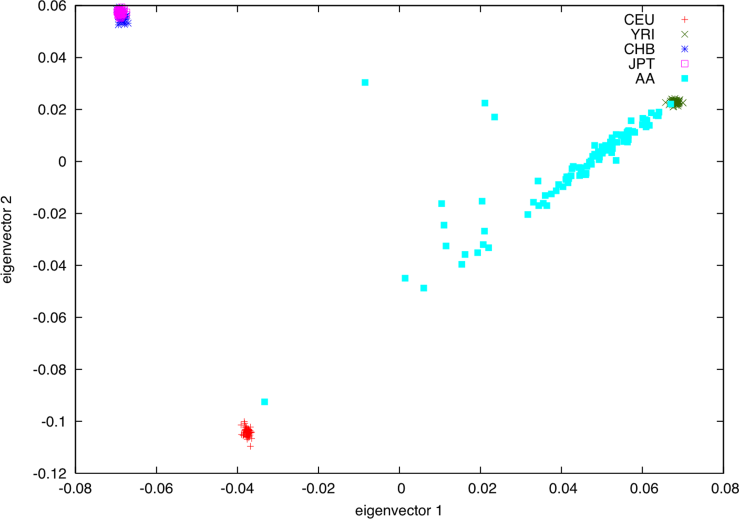
(Price, 24)
The majority of mitochondrial haplogroups (mtDNA) that African Americans have are African, since these come from African women originally, “… individuals with L, U6, or U5b1 haplogroup mtDNA and primarily African nuclear ancestry were defined as having low levels of divergent ancestry, whereas individuals with non-African haplogroups and high degrees of African nuclear ancestry had high levels of divergent ancestry.”(20) These researchers looked at any potential confounding variables that would skew results for the African American population. They examined a number socioeconomic variables such as years of school taken, income, etc. According to the researchers, “There was no detected statistical association between divergent ancestry and any of these factors.” (21)
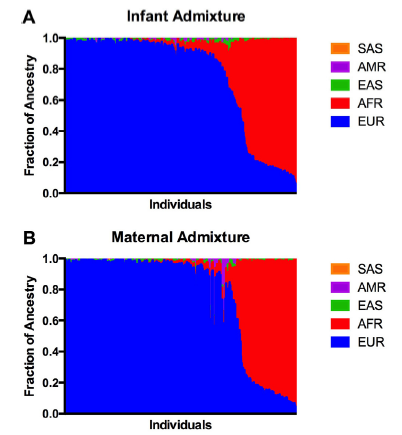
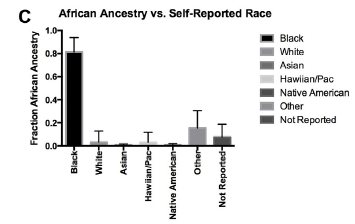
Measurements of Admixture For Test Subjects
South Asian[SAS], American [AMR], East Asian [EAS], African [AFR] and European [EUR]
(Crawford, 20)
Crawford et al go on to establish that the mitochondria functions are disrupted because mtDNA and yDNA haplogroups typically co-evolved in certain populations. European and African haplogroups really aren’t supposed to be together in one cell based on this observation. And this reality extends to other non-human organisms as well, “Animal studies have shown that common haplogroup polymorphisms have consequences for reproductive fitness. In this study, we have found that the inheritance of nuclear and mtDNA from distinct ancestral origins is associated with an increased risk for preterm birth.”(20) And, “In livestock, certain mtDNA haplotypes are associated with improved milk and meat quality, whilst, other species, mtDNA haplotypes have shown increased longevity, growth and susceptibility to diseases.”(26) These observations from animals bolster the case for mtDNA interaction for discordant ancestry in humans. This is the case even though farm animals and humans won’t have the exact same outcomes as they aren’t the same species. The same logic can be applied to epigenetic phenomena as well: we should expect epigenetic phenomena in humans because we observe them in other species (like mice). But that in no way guarantees that we would observe the same or similar overreaching trait modifications. Other studies of animals have revealed that this trend of cross breeding distinct populations causes changes health outcomes in multiple ways, “…mitochondrial haplogroups have been bred into a distinct nuclear background, also show the potential for widespread changes in health, with the incidence of obesity, insulin signaling, and lifespan all affected.” (20)(25)
But what does this have to do with New York biracial infants? Simple: the rates of preterm infants born to Hispanic fathers/White mothers and Black fathers/White mothers are exactly the same, which is at 1.4. That is worse than the healthiest White average of 1. For Hispanic mothers/White fathers, the rate was at 1.5. Hispanic people have high amounts of discordant ancestry from Africa, Europe, and Native Americans,”… Latinos in the US carry 18.0% Native American ancestry, 65.1% European ancestry, and 6.2% African ancestry.”(20) So, Crawford et al’s findings readily apply for these Hispanic/White offspring: their poor outcomes can be partially explained by the all the African, Native American, and White ancestry that they have.
As previously stated, I am in no way denying that maternal poverty or stress has an effect on infant health. The most recent, credible research shows that depression absolutely affects an infant during gestation,”…infants from depressed mothers were found to have increased methylation of the NR3C1 gene compared to infants from non-depressed mothers.”(28) However, the “stress hypothesis” cannot not be applied for all members in discordant relationships, or count for all/most the effects that occur in biracial births. Nor I do I believe that the environment is primarily responsible for these outcomes. The main problem with this proposition is that many White Americans already approve or don’t mind interracial marriage. But White people aren’t marrying out as much as other ethnic groups. Therefore, in the rare instance that a White person has a non-White partner, it is unlikely that these interracial couples are being treated in a less-preferable way by their families:
“…Whites are somewhat less willing to marry and bear children interracially than to date interracially. These attitudes and behaviors are related to warmth toward racial outgroups, political conservatism, age, gender, education, and region. Third, White women are likely to approve of interracial relationships for others but not themselves, while White men express more willingness to engage in such relationships personally, particularly with Asians. However, neither White men nor White women are very likely to actually engage in interracial relationships. Thus, positive global attitudes toward interracial relationships do not translate into high rates of actual interracial cohabitation or marriage despite the fact that most White Americans (especially White females) aren’t interested in being in a relationship with a non-White person.” (5)
In fact, different races/ethnicities do not experience the same amount of stress while they are in an interracial relationship. And this spans across different age groups, “The negative effects of interracial dating hold similarly for boys and girls and among White and Black youth. Interracial dating less negatively effects the depressive symptomatology of Hispanics, though, and actually appears to ‘protect’ Asian youth from depressive symptoms.”(9) Additionally, White women seem to get extremely stressed from being in a relationship between either Hispanic or Black males. Blacks in those relationships aren’t affected by stress in those relationships:
“…non-Hispanic whites intermarried with non-Hispanic blacks, non-Hispanic whites intermarried with non-Hispanic other races, and non-Hispanic white women with Hispanic husbands report significantly poorer health than their endogamous counterparts. Furthermore, non-Hispanic whites with non-Hispanic black spouses also fare worse than their interracially married peers with Hispanic spouses. In contrast, the self-reported health of married non-Hispanic blacks shows no significant difference between the interracially and the endogamously married.”(10)
These were based on self-reports. One could even say that the problem with self-reports is that there could be bias with what an individual is actually reporting; in terms of how people are treating them, there very well could be exaggerations or dishonesty. There is the reality of perceived discrimination, i.e. the perception of being discriminated regardless if it is really happening. (15) It is true that Borrel et al speculate that stress contributes to the poor health of mixed infants, “Moreover, partnering with a man outside a woman’s race/ethnicity may lead to stress because of discriminatory treatment, family disapproval, and reduced social support.”(4) They reference an older study entitled “What about the couple?’ Interracial marriage and psychological distress.”(8)
This study explored the stress levels of interracial couples, especially of Native Americans, Hispanics, and White people. Indeed, the stress levels of poverty were observed, “Lower socioeconomic status explains approximately half of the increased distress experienced by white women, while higher socioeconomic status partially suppresses increases in distress for Hispanic men and women.” (8) I am not aware of any demographic data that shows all/most White American parents shun their children that engage in an interracial relationship. If someone is going to try to debunk the apparent genetic contribution to poor health outcomes via stress through neglect, they would need to show that this is an overreaching factor for all/most of these relationships.
Where this stress is coming from is another important aspect to consider: Even if there was a trend of neglect for interracial families/pregnancies, it would only be because of the natural inclination to find these relationships unacceptable, “Bias against interracial romance is correlated with self-reported feelings of disgust”. (12) This phenomenon can be observed via brain scans. There is an intense neural mechanism that is triggered when a person observes interracial couples,“Interracial couples elicit a neural disgust response among observers — as indicated by increased insula activation.”(12) In this case, this psychological disgust could be considered an extension of ethnic nepotism or association; if people are disgusted by these relationships it would imply that being involved with an individual of an out-group is not beneficial to the in-group. Because the affects of race mixing create unhealtheir children, this natural disgust is moral. And as I have shown above, the most distinctive evidence proves this.
Objection 2: What about Asians in NYC ? They are some of the most impoverished people in the city. How can you assume it’s not mostly/entirely the impoverished environment that’s causing these problems?
Despite the fact that 40% of all NYC Asians were low-income earners in the early 2000’s, 60% of Asians living in the city were not living in poverty.(7) In other words, the majority of these Asians were not low-income earners. Another problem with this objection is that the vast majority of these people were also not of child rearing age; most of the Asians living in poverty were either seniors or children.(7) (In this case, young teenagers are considered children.) Cambodians seem to have highest rates of poverty, but I am not aware of any surge interracial relationships between Cambodians and out-group races.(7) Therefore, young Asian adults are probably the ones who engage in a ethnically discordant union, regardless of the pairing. Case in point, it’s critical to look the actual demographic data:
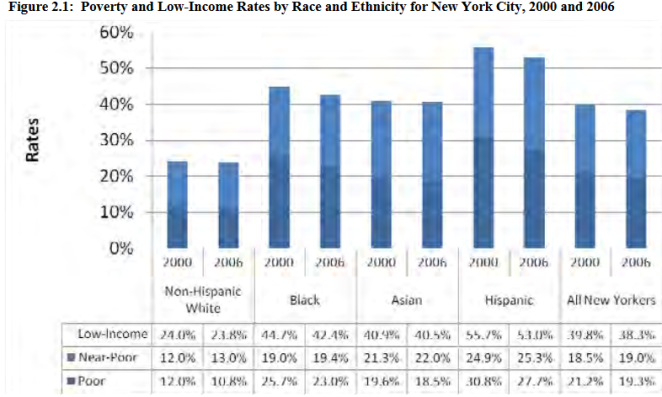
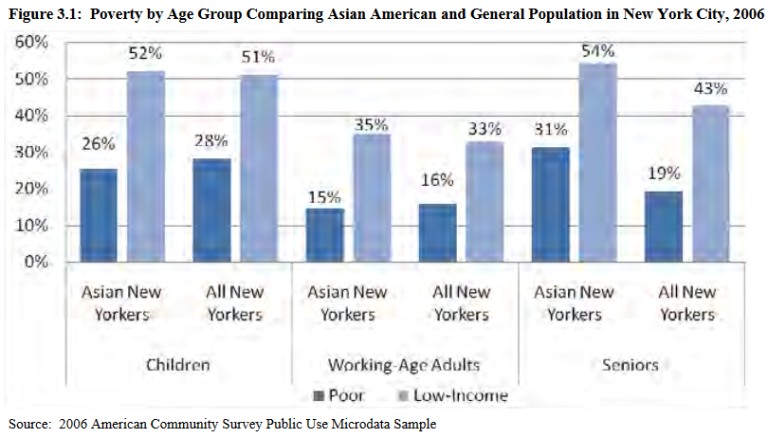
Furthermore, the rates of poverty for NYC Asians has been free falling since the year 2000. It is incoherent, therefore, to assume that poverty is the sole cause for poorer healthcare outcomes for these half-Asian children. (1) Again, how one defines an influence that accounts for “most” outcomes depends on perspective. As for poverty, again I would simply conclude that it is important but alas, not the only factor. When we look at the whole country, the vast majority of Asians aren’t living in poverty either. (3)
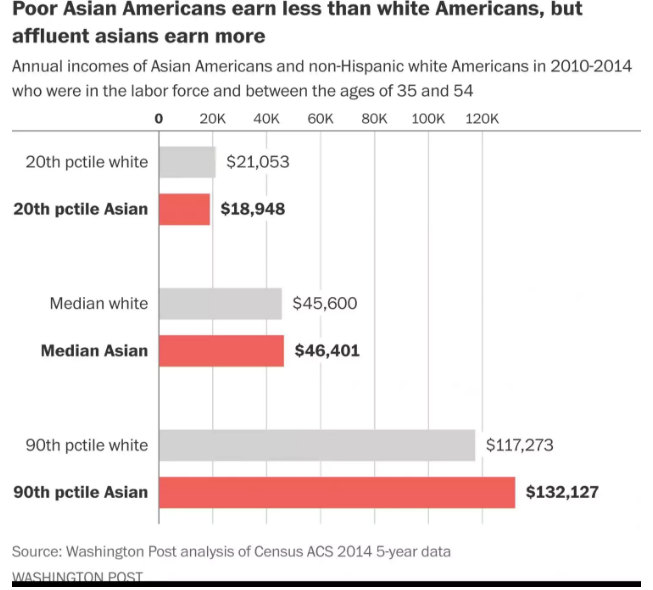
(Guo, 3)
Finally, we have evidence from a recent infant study that evaluated the health of Korean biracial infants. Yang et al proved that the genetic underpinnings of mate choice in poor health outcomes. These researchers looked for similar ailments as reported in the New York study: low-birth weight, high birth weight, preterm births, “This study evaluated pregnancy outcomes according to parental ethnicity and found significant differences in birth weight between the study groups, with the highest birth weight in the Foreign Father and Korean Mother (FFKM) group and the lowest birth weight in the Korean Father Foreign Mother (KFFM) group.”(33) Korean men who had biracial offspring typically married women from South Asia. The genetic distance between South Asians (India, Pakistan, Bangladesh, etc) and East Asians is actually quite high. And as far as I am aware, these individuals weren’t poor either, since majority of people living in poverty in South Korea are elderly, “The limited scale of pension provision and social welfare explain why nearly one-half of the elderly live in relative poverty, the highest proportion among OECD countries.”(29) It’s necessary to look at PCAs to show the genetic relatiblity among East Asian populations:
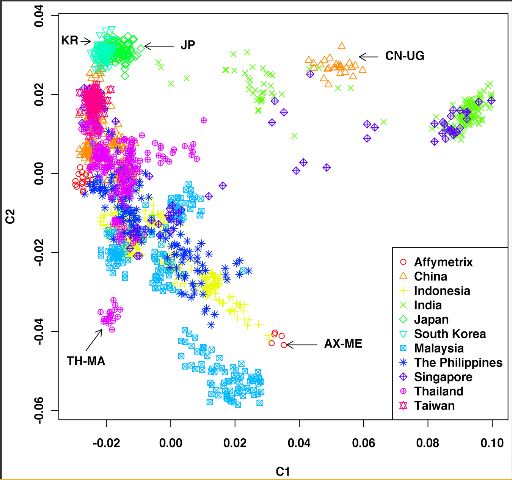
(Yang, 31)
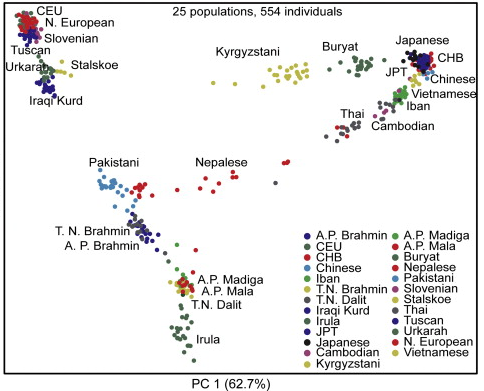
(Xing, 19)
Notice that there are various clines and clusters that represent the genetic diversity within India. T.N. Brahmin,A.P. Brahmin, Pakistani clusters/clines are quite far away from the Japanese and Chinese clusters respectively. The first PCA from Yang et al shows that Koreans are very close to other East Asians:
“In Korea, most Korean men in an interracial marriage chose to marry Asian women, particularly those from Southeast Asia, who are generally smaller than Korean women; in contrast, most Korean women in an interracial marriage chose to marry Western men, who are generally taller than Korean men. Birth weight is known to be associated with parental genetic factors. In addition, our results suggest that foreign fathers generate a “promoting effect” on birth weight in the offspring of Korean mothers, whereas foreign mothers generate a “constraining effect” on birth weight in the offspring of Korean fathers, similar to the findings in a study by Wells et al. Based on their study, the results of paternal ethnicity differences between two ethnic groups were asymmetrical, which suggests ‘paternal-promoting’ and ‘paternal-restraining’ effects.”(33) The mate choice for Korean men are smaller women while Korean women choose are larger men, “Maternal and paternal height represent a complex conjuncture of genetic and environmental influences, especially long-term dietary intake and nutritional status.”(34) The genetic/environmental heritability of height can be explored further by comparing shorter populations to larger ones, such as Pygmies and Bantus.(35)
Objection 3: Since Asian teenagers and seniors are extremely impoverished and live in polluted housing, how do you know that they aren’t having interracial children?
It’s unlikely that most Asians with interracial children are having pregnancies below the age of 20, considering the fact that they currently have the lowest rate of teen pregnancies overall in the city. (2) The rate of teen pregnancies for Asians was already one of the lowest in NYC, and the rate even began to free-fall from 2000 to 2011. I am not aware of any demographic evidence that suggests Asian teens were having interracial children in large numbers, especially in the early to the late 2000’s.

As for Asian seniors, I am not aware of any demographic evidence that they are having children at that age.
Objection 4: “What about pollution causing low-birthweight? Pollution in the city could cause this lower birth weight, which would be contrary to that ailment is influenced by genetic inheritance.”
Levels of pollution certainly can affect birth weight, but this depends on the geographic context and the chemical involved. Consider Massachusetts. There is medical evidence that exists for infants born in that state having a higher rate of low birth weight, specifically from pollution.(23) For New York, there is currently no consistent evidence that ozone affects a child’s likelihood of low birth weight, “There were no consistent dose-response relationships between the pollutants and TLBW (term low birth weight). Ozone exposure was associated with a higher risk of TLBW only in the first trimester, but these results were not statistically significant. Exposure to the third quartile of ozone for the full gestational period had negative associations with TLBW (odds ratio = 0.86; 95% confidence interval, 0.81-0.92).”
And finally, “Collaboration within the Environmental Public Health Tracking Network to share methods and data for research proved feasible and efficient in assessing the relationship of air pollutants to adverse birth outcomes. This study finds little evidence to support positive associations between exposure to ozone or PM2.5 and TLBW (term low birth weight) in New York State.”(21) One study,“…found a statistically significant association between PbB and birth weight. Relative to 0 μg/dL, PbBs of 5 and 10 μg/dL were associated with an average of 61-g and 87-g decrease in birth weight, respectively.” Also that study found that, “Low-level PbB was associated with a small risk of decreased birth weight with a supralinear dose–response relationship, but was not related to preterm birth or small for gestational age. The results have important implications regarding maternal PbB.”(32) Considering how small the reduction of weight was for the offspring itself, maternal blood lead level had an extremely small effect on these infants. Healthy birth weight for infants overall is at least 2500 grams, and 61 and 87 grams is minuscule in comparison.(4)
Sources
- http://www1.nyc.gov/assets/opportunity/pdf/NYCgovPovMeas2017-WEB.pdf New York City Government Poverty Measure2005–2015
- https://www.cccnewyork.org/wp-content/uploads/2013/11/DOHMHPresentation.pdf Teen Sexual and Reproductive Health in New York City
- https://www.washingtonpost.com/news/wonk/wp/2016/12/20/why-asian-americans-arent-as-rich-as-they-seem/?utm_term=.94a0fc8c4ecf The staggering difference between rich Asian Americans and poor Asian Americans
- Parental Race/Ethnicity and Adverse Birth Outcomes in New York City: 2000–2010 Luisa N. Borrell, DDS, PhD, Elena Rodriguez-Alvarez, PhD, David A. Savitz, PhD, and Maria C. Baquero, PhD, MPH
- I wouldn’t, but you can: Attitudes toward interracial relationships https://www.sciencedirect.com/science/article/pii/S0049089X11001815
- Gestational duration and birthweight in White, Black and mixed-race babies http://onlinelibrary.wiley.com/doi/10.1111/j.1365-3016.1991.tb00724.x/full
- Working but Poor: Asian American Poverty in New York City, Asian American Federation http://www.aafny.org/doc/WorkingButPoor.pdf
- What about the couple?’ Interracial marriage and psychological distress https://utmb.influuent.utsystem.edu/en/publications/what-about-the-couple-interracial-marriage-and-psychological-dist
- The role of family relationships in the psychological wellbeing of interracially dating adolescents http://www.sciencedirect.com/science/article/pii/S0022103116300555
- Interracial Marriage and Self-Reported Health of Whites and Blacks in the United States https://link.springer.com/article/10.1007/s11113-017-9438-0
- Prematurity and Low Birth Weight as Potential Mediators of Higher Stillbirth Risk in Mixed Black/White Race Couples https://archive.is/j1nW1#selection-471.0-471.115
- “Yuck, you disgust me!” Affective bias against interracial couples https://www.sciencedirect.com/science/article/pii/S0022103116300555
- The epidemiology of alcohol, marijuana, and cocaine use among women of childbearing age and pregnant women. http://europepmc.org/abstract/med/8513621
- Epigenetic regulation of Newborns’ imprinted genes related to gestational growth: patterning by parental race/ethnicity and maternal socioeconomic status http://jech.bmj.com/content/early/2015/02/12/jech-2014-204781
- Perceived discrimination in U.S. healthcare: Charting the effects of key social characteristics within and across racial groups https://www.sciencedirect.com/science/article/pii/S2211335515000972
- Geronimus AT. The weathering hypothesis and the health of African-American women and infants: evidence and speculations. Ethn Dis. 1992;2(3):207–221.
- Nuru-Jeter A, Dominguez TP, Hammond WP, et al. “It’s the skin you’re in”: African-American women talk about their experiences of racism.
- Braveman P. Black–white disparities in birth outcomes: is racism-related stress a missing piece of the puzzle? In: Lemelle AJ, Reed W, Taylor S, eds. Handbook of
African American Health Social and Behavioral Interventions. New York, NY: Spring; 2011:155–163. - Xing, Jinchuan, et al. “Toward a more uniform sampling of human genetic diversity: a survey of worldwide populations by high-density genotyping.” Genomics 96.4 (2010): 199-210.
- Bryc, Katarzyna, et al. “The genetic ancestry of african americans, latinos, and european Americans across the United States.” The American Journal of Human Genetics 96.1 (2015): 37-53.
- Crawford, Nicholas, et al. “Divergent patterns of mitochondrial and nuclear ancestry are associated with the risk for preterm birth.” The Journal of pediatrics(2017).
- Bell, Michelle L., Keita Ebisu, and Kathleen Belanger. “Ambient air pollution and low birth weight in Connecticut and Massachusetts.” Environmental health perspectives 115.7 (2007): 1118.
- Brown, Jessica M., et al. “Linking air pollution data and adverse birth outcomes: environmental public health tracking in New York state.” Journal of public health management and practice 21 (2015): S68-S74.
- Price, Alkes L., et al. “Effects of cis and trans genetic ancestry on gene expression in African Americans.” PLoS genetics 4.12 (2008): e1000294.
- Latorre-Pellicer, Ana, et al. “Mitochondrial and nuclear DNA matching shapes metabolism and healthy ageing.” Nature535.7613 (2016): 561.
- Tsai, Te-Sha, Sriram Rajasekar, and Justin C. St John. “The relationship between mitochondrial DNA haplotype and the reproductive capacity of domestic pigs (Sus scrofa domesticus).” BMC genetics 17.1 (2016): 67
- Tong, Shilu, Peter Baghurst, and Anthony McMichael. “Birthweight and cognitive development during childhood.” Journal of paediatrics and child health 42.3 (2006): 98-103.
- Provenzi, Livio, Elena Guida, and Rosario Montirosso. “Preterm behavioral epigenetics: A systematic review.” Neuroscience & Biobehavioral Reviews (2017).
- OECD Economic Surveys KOREA APRIL 2012 OVERVIEW https://web.archive.org/web/20121203014227/http://www.oecd.org/eco/50191444.pdf
- 1. Trends and patterns in intermarriage http://www.pewsocialtrends.org/2017/05/18/1-trends-and-patterns-in-intermarriage/
- Yang, Xiong, Shuhua Xu, and HUGO Pan-Asian SNP Consortium. “Identification of close relatives in the HUGO Pan-Asian SNP Database.” PloS one 6.12 (2011): e29502.
- Zhu, Motao, et al. “Maternal low-level lead exposure and fetal growth.” Environmental health perspectives 118.10 (2010): 1471.
- Yang, Sun Young, et al. “Analysis of Pregnancy Outcomes among Interracial Couples in Korea.” Journal of Korean medical science 32.10 (2017): 1657-1661.
- Troe, Ernst-Jan WM, et al. “Explaining differences in birthweight between ethnic populations. The Generation R Study.” BJOG: An International Journal of Obstetrics & Gynaecology 114.12 (2007): 1557-1565.
- Jarvis, Joseph P., et al. “Patterns of ancestry, signatures of natural selection, and genetic association with stature in Western African pygmies.” PLoS genetics 8.4 (2012): e1002641.
* * *
Source: European Survival
For further reading:




{kind=link}
[…] Mixed Race Infants are Unhealthy Because of Complex Gene-Environment Interaction […]
how do we know haplogroups are real and its not just a jewish hoax
What my working hypothesis is according to definition and etymology of the term “semite” is. “Semites” are the result of a previous conquest of white man. So in essence some white’s through dna disobedience went outside into whatever native groups they ran across. Examples in modern world by simple observational facts, latin america, middle east, India. Results are the same browner toned people. The jews have realized this and since tried to remove the brown skin.